

Bravo! Anticipated Changes in Healthcare Financing!

Healthcare reform is generating a lot of angst among the CFOs of large businesses feeding off the exorbitant costs of healthcare in the U.S. One such company is Ensemble Health Partners, which extols its revenue cycle management and has posted an article on LinkedIn reviewing suggested reforms for four healthcare policies. Wiki defines revenue cycle management as "all administrative and clinical functions that contribute to the capture, management, and collection of patient service revenue."
The Ensemble article cites concerns about four anticipated policy changes:
Removal of ACA enhanced subsidies,
Changes to Medicare Inpatient-Only list,
Personnel changes driving volume to Medicare Advantage plans, and
Expanded use of site-neutral payments.
These suggested changes in the healthcare financing system would greatly improve healthcare affordability, but are of concern to Ensemble because of the loss of hospital income which would result from these changes.
1. Removal of ACA Enhanced Subsidies
The Ensemble article notes that the subsidies to make the Affordable Care Act feasible for low-income patients are set to expire at the end of 2025. Ensemble notes that without these subsidies, the cost of premiums could increase more than 75 percent, leaving many patients unable to afford the insurance. The Ensemble focus is on the loss of revenue this would cause providers rather than the problem of a large portion of the patient population being unable to afford health insurance.
2. Changes to Medicare Inpatient-Only List
Medicare has a list of procedures which it will only pay for when done in hospitals. Many of these procedures could be performed in clinics. What's more, many of these procedures could be provided for much less money in clinics. As Ensemble notes, if legislation is passed to have Medicare pay for these procedures in other than hospital settings, hospitals will lose a significant revenue stream.
Years ago, I could do a procedure called a cervical cone biopsy. It was named after its shape and had the advantage of being both diagnostic and therapeutic for early cervical cancer. We were taught that we were required to please the pathologist, in other words, extract a big cone. The downside to that way of thinking was the bigger the cone, the more trouble for the mother. Removing a large cone could weaken the cervix. Weakening a woman's cervix can lead to preterm cervical dilation and preterm birth. Indeed, sometimes the cervix would became stenotic and would not dilate at all.
So, to avoid all of this injury to mothers, I started being conservative and doing smaller cones. After all, why please the pathologist and cause unnecessary injury to the mother whose pregnancy career could be permanently affected adversely by the cone treatment. To that end, I soon discovered that the smaller cone could easily be done in the office for $85 compared to the $4000 cost in the hospital. The problem was that the insurance companies could not get their heads wrapped around significant cost savings. The even greater cost saving was the prevention of the birth of premature babies born at 22 weeks because of cone damage to the mother’s cervix. Care for such a premature baby costs thousands of dollars over the baby’s lifetime. Performing smaller cones in my office saved payers millions of dollars.
Sometimes in healthcare it is necessary to think long-term, something our present billing and coding systems either can’t or won’t do. This is not to say that looking ahead can’t be done. It is rather to say that the people presently in charge have chosen by default not to look at the results of failing to look ahead. Those responsible for Medicare decisions about hospital only procedures, wedded to inpatient-only lists, have perpetrated a seriously undesired result driving up healthcare costs.
The thought that this discrimination against clinics was wasting large sums of money appears to have never occurred to Medicare or Medicaid.
Let's face it. Payment for a procedure should be the same whether done in a hospital or a clinic.
3. Personnel Changes Driving Volume to Medicare Advantage Plans
Medicare Advantage plans are notorious for significantly increasing the cost to the government and these plans deny claims twice as much as commercial plans. I can certainly agree with Ensemble that the so-called Medicare advantage plans are a disaster!
These plans are much worse than the article would lead you to believe as I noted in "Medicare So-Called "Advantage Plans." Or in "What's the Advantage in Medicare Advantage Plans? These plans cost Medicare $88 billion per year. Right now they are, without a doubt the single biggest debt in the Medicare healthcare budget, probably more than all the other budget problems put together. These plans should be eliminated ASAP. They are now dropping entire communities from their roles. They are also dropping high acuity patients who need to return to Medicare (Traditional Medicare) from MA plans.
4. Expanded Use of Site-Neutral Payments
The term site-neutral means Medicare would be required to pay the same rate for services delivered regardless of where the care is delivered. Payments for the same care are different depending upon where the care is provided. Payment for care in the emergency room will be reimbursed at a higher rate than that same care provided in a doctor's office. Ensemble suggests hospitals could $5 million or more annually if site-neutral payments are implemented.
The onerous task of providing healthcare payments for those who are underserved and cannot afford healthcare falls to state Medicaid departments. Although Medicaid carries the weight of the Federal and State governments, their burdensome machinery moves slower than glaciers. In my medical career I’ve spent many frustrating years dealing with payers, and by far the worst, both in terms of deliberately denying claims but also in terms of failure to recognize good care goes to Medicaid.
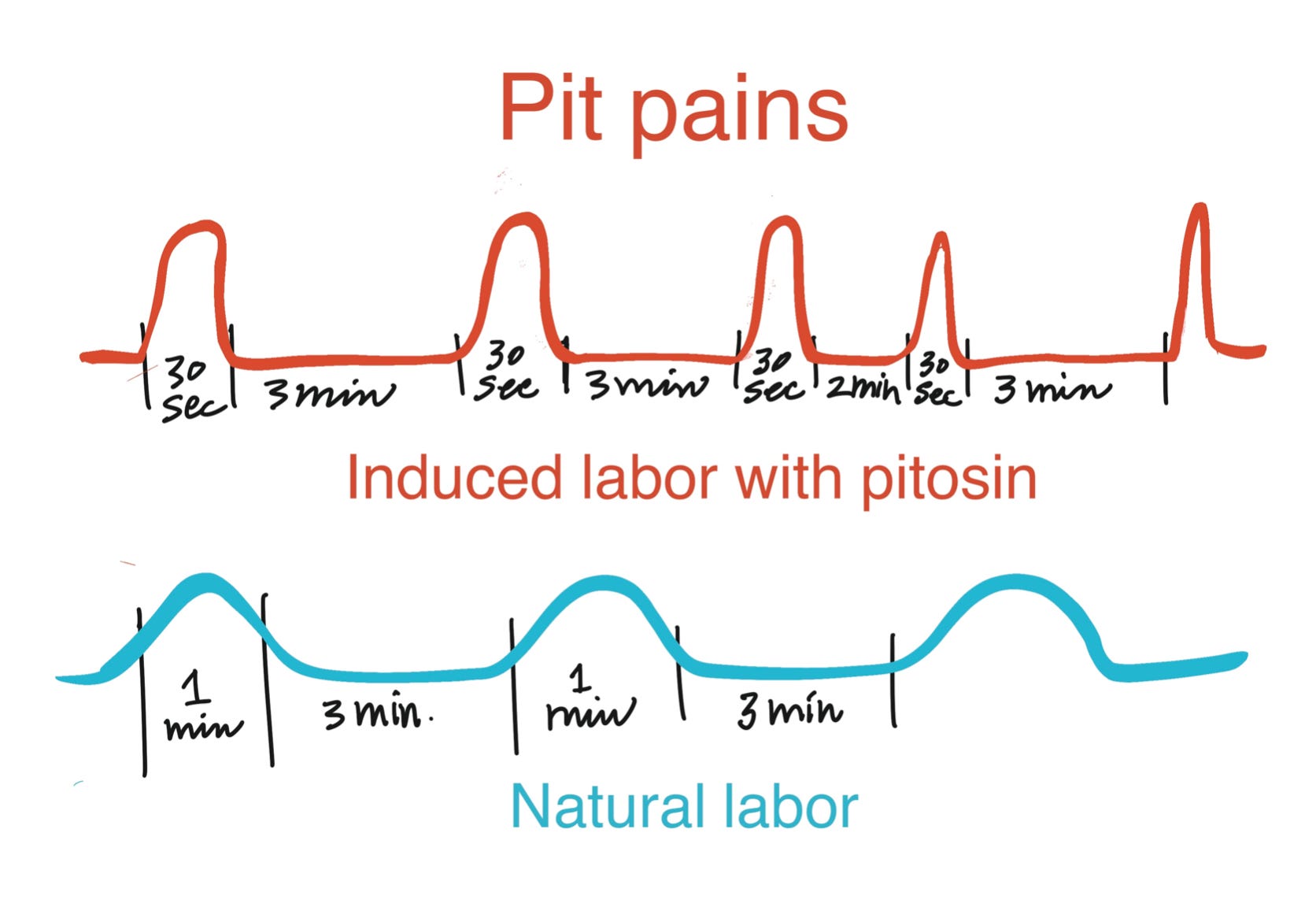
I have always hated the standard form of labor induction. The patient goes to labor and delivery, undresses, gets IV Pitocin, and an amniotomy (amniotic sac is broken). The patient will get an epidural because the pitosin pain is extreme, much more severe than natural labor. Pitocin pain is called pit pain.
What we don't know is what effect the severe contractions resulting from pit pain have on the baby. The baby can’t tell us about pain. I have never supported the idea that it’s OK to use the head of the baby in the uterus as a battering ram. Nature does not do this. There has never been a study telling us anything about the effects of this procedure on the baby. We don’t know whether it’s safe or harmful and have no parameters for it. So, we have foolishly assumed, without evidence, that this procure is harmless.
Four decades ago I found that prostaglandin is very different from oxytocin. Prostaglandin is what nature uses to get the mother’s uterus and cervix ready for labor. Prostaglandin contractions are small and frequent and either don’t hurt at all or feel like period cramps. You see, Mother Nature is very sensible. She gets the cervix ready first and then starts serious labor by adding oxytocin when a mother's cervix is dilated about six centimeters. Mother Nature says open the garage door and then drive the car out. There’s no sense trying to drive through the garage door.
Even forty years ago, labor inductions in the hospital could cost $4000. Payment was site-specific. Inductions were only paid for in hospitals. Then you could add an emergency C-section for $3,000 for the labor failing to progress. Because there was no billing code for office, induction payers would not pay me for any part of an induction in my clinic. I charged $125 for fetal monitoring. I used a very small dose of Cytotec in my office to do what is called cervical ripening. If this small dose (25 mg) of Cytotec softened the cervix and readied the mother for delivery, she could go home and wait for delivery to start in earnest and go to the hospital for delivery. If the baby was not ready for delivery, the Cytotec did not cause the cervix to thin. However, if the mother had gone to the hospital and been started on pitocin and her cervix did not thin and prepare for birth, the mother was kept in the hospital and continued on pitocin and eventually diagnosed with "failure to progress." She would not be allowed to return home and wait for nature to take its course. Instead, she would be kept in the hospital and undergo an emergency C-section. Using Cytotec in my office to prepare the cervix for delivery prevented C-sections. This saved insurers, including Medicaid, not only $4000, but resulted in the delivery of a healthy term baby without excessive interventions. This saved payers millions of dollars
Since the office Cytotec was so much cheaper and much more effective, the payers could have chosen to pay for the cervical ripening in my office as part of induction, making the procedure site neutral.
Making procedures such as cervical ripening site-neutral prevents the public and providers from being forced to pay for hospital procedures when those procedures could just as safely be provided in clinics at great cost savings.
Time for These Long Overdue Changes in Healthcare Financing
Aside from the Medicare Advantage plans, which are a dangerous 88 billion-dollar per year boondoggle, most of these anticipated changes discussed by Ensemble are either neutral or help bring down healthcare costs to consumers. Corporate hospital business practices have been driving up the cost of care for the past 40 or 50 years.
So far, it would be super to see the next four years usher in some social consciousness from our legislators who could put the brakes on Big Pharma and big business lobbyists further destroying our dysfunctional healthcare system.
P.S.: When I support a writer, I personally prefer donations to subscriptions. Subtack does not offer the donation option for writers. At LindemannMD.com, there is a donation option for the Safe Pregnancies Foundation in the sidebar widgets. Donations welcome! Thank you.